
Trauma of Identity
The trauma of identity means that I am not able to be myself; I lose my true identity in the moment in which this trauma happens. My survival of this trauma at that earliest time of my life, usually pre-birth, meant that I had to give up on my wants, my identity, and identify with the wants and needs of my mother, with her identity instead. We call this identification. This is the strategy for surviving a Trauma of Identity.
To exist is to have needs... and wants. They are different of course: needs are about baseline survival in whatever context; all living things have basic needs without which they will die: air to breathe, food, safety, warmth, metabolic processes (digestion and excretion), and the primal urge to procreate and contribute to the perpetuation of the species. These needs are about basic life survival... not trauma survival. If these basic physical needs are not attended to, the being will die.
These are also the needs of the baby, and as vulnerable and dependent as she is, she also has emotional and social needs: the need for love, emotional and physical contact, to be seen for the unique and integral being that she is, to experience respect and value for her wants, to be allowed to explore her world as she wishes while being held in a safe environment to do so. If the child can experience these things in her first relationship, that with her mother, she can grow into an autonomous, self-authorising, self-responsible adult.*
To exist is also to want. There is no real existence without wanting. To have an identity is to have valid and personal wants; they are the child’s wants, specific to her and to do with her sense of who she is. They are in a sense her identity, her sense of being able to be herself. She cannot really be herself if she does not want, for herself. In a way her own clear personal wants define her and are in that sense her identity.
As a baby, the child’s existence is fragile because she is utterly vulnerable and dependent on her mother. Her mother is her life and the source of her existence. This is in a very physical way - while in the womb she does not survive without her mother’s continued physical existence - but it is also in an emotional way: she needs her mother to see her as a unique individual in order to be one. She needs her mother to respect, understand and respond to her wants, as, fragile, uncertain and emerging as they may be.
If this is not possible, if the mother has her own agenda, puts her wants first, sees the child as a means to her own personal ends, her own gain, perhaps even doesn't 'want' the child, this all must override, ignore and treat as non-existent the fragile, tenuous wanting identity of the infant. The child cannot fight it; he can only succumb. Without a thought, because thinking is not yet developed, the infant gives up. He can do no other than relinquish himself, his identity, his wanting self... it is not a choice. The mother has all the power consciously and unconsciously, and the infant, without a whisper, must comply.
This is the trauma of identity, the loss of self, the loss of connection to personal wanting, and the only option for the child is to fill the vacuum left by identifying with his mother's wants... her wants dominate and become his wants. Thus the mother is a perpetrator, and the child an innocent victim.
And, from this moment the infant, by aligning himself with his mother's wants, is forced to become a perpetrator to himself; from this time the endeavour becomes to abolish, suppress or feel guilty about his wants, and by doing this he is against himself. He (or she of course) is the negator of his own identity; he kills himself off. He can be himself no more. Here we find adults who do not know what they want, can only find wanting through identification with others' wants, are frightened of their wanting urges, suppress and avoid wanting and instead take care of others' wants. This self-perpetration even becomes manifest in physical self-injuring, self debasement, sometimes even resulting in the ultimate self-perpetration, suicide.
Or we may find adults who have identified so much with the perpetrator/mother that they force their wants on others, becoming perpetrators and bullies to others in a dreadful replication of their own childhood experience at the hands of their mother.
The Trauma of Love
Hand in hand with the Trauma of Identity goes, of course, a lack of love. A mother who is able to truly love her child is a mother who can see and respect the child's wanting self. A mother who does not see and respect the emerging wanting identity of the child cannot love. Love is an absolute, an emotional experience that is generous, open, respectful and free. It makes no demands and it honours the other as a free, whole, autonomous entity.
So the Trauma of Identity breeds and implies a Trauma of Love. The child cannot gain a free, loving connection with a mother who puts her wants above those of her child; she is not available for real love in a consistent way.
Trauma survival forces the psyche of the traumatised person to split. This is important to understand in light of the above for one reason: if we have survived trauma we are split in our psyche and that means that our ability to be in the world is compromised, variable and inconsistent.
This means that however traumatised a person is, there is even so always still available a healthy part, a healthy 'I', and from this healthy 'I' the person is able to feel clear and honest emotions, including love. The difficulty is that much of the time the person will be more in their trauma survival self, and as such real love is not possible; it can only be a 'survival', often manipulative, form. It may be attempts at love, or distortions of love, but these cannot be love: manipulation is not love.
The way in which we survive this trauma of love is by taking on others' delusions of love, of which there are an infinite variety - and even developing our own - such as: 'love heals everything'; 'if I am really good my mother will love me'; 'money can buy love'; 'I can make someone love me'; 'If I can just find the right clothes, hair cut, make-up, shape (etc) then this person will love me'.
So now we have a child with a Trauma of Identity and a Trauma of Love.
Trauma of Sexuality
We all know that hypothetically the sexual act is meant to be an expression of love and connection between two people; a highly intimate, vulnerable and embodied expression of love. But this is not how many of us experience or engage in sex and sexuality. We only have to look carefully at the majority of our advertising and selling strategies to understand how sexuality is manipulated and commodified.
If a child has suffered a Trauma of Identity and is not clear who he is, having lost connection with his wants, and has additionally suffered a Trauma of Love, and so has delusions of loving, believing that his (perpetrator) mother loves him, or that he can make her love him, what then happens to his sexuality, his ability to express love and intimacy with a partner?
And worse still, if the context in which the child has to spend the early part of his life is an unsafe, traumatising environment, with parents who are themselves traumatised and confused about important things like identity, love, safety, power and sexuality, and they live out their confusion and distortions on a daily basis with their children, there is the setting for escalating violence and the appropriation of sexuality as a weapon to victimise, punish, misuse and abuse.
Sexuality becomes objectifying, abusive and coercive, as divorced from love as it is possible to be.
Recently Franz Ruppert, the developer of these ideas about trauma and trauma healing (as Identity-oriented Psychotrauma Therapy), came up with the notion of our Traumabiography. By this term he is indicating this trio of traumas, of identity, love and sexuality, or another way of putting these traumas is by their manifestation: the child is unwanted, unloved, unprotected. The traumabiography looks like this:
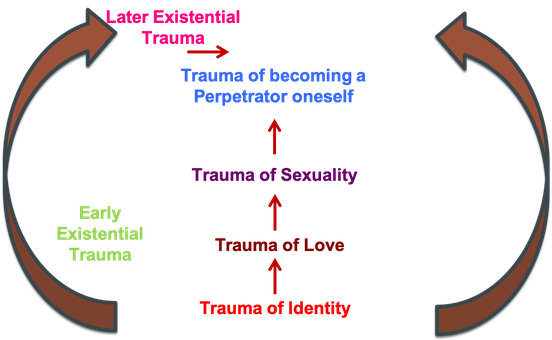
The important thing to understand about this traumabiography is that it is our biography and we live our lives through this biography every day.
************
I started out to write about what I see as the general progression of healing from these early traumas. It seems that in order to do this I needed to write about these traumas in as stark a way as I could.
The reason is that I see the process of those I work with usually taking quite a specific course, which I can recount as follows:
Being willing to explore the possibility that this method might help
For many this may be a last-ditch attempt to address issues that they know are there and other forms of therapeutic process have not changed or addressed.
A persistence of current gained perceptions and meanings...
... or to put it another way a difficulty with opening to see something new. This is entirely predictable since our instinctual and natural way of dealing with traumatisation is to avoid, deny and suppress, usually creating palatable stories to explain away our symptoms and concerns. We cling to these threads of meaning-making as to a life-belt, but they often can prevent us from seeing beyond. Combined with this is an unconscious and deep sense of loyalty to the stories fabricated by our family that also avoid difficult and painful truths. Our parents and family may try to protect us, but often also are protecting themselves from their own discomfort and trauma pain.
A creative mix of the recognisable and known, along with new insights and perceptions.
This begins as the person starts to trust the process (and the facilitator), and gains a growing trust in themselves and their unconscious and semi-conscious knowings that more frequently surface in the work.
Increased contextual reality.
The previous phase then becomes a phase of seeing and recognising with greater perception and understanding the reality of the context in which the person arrived as an infant, and had to survive. This is often shocking, even if already known on some level... it is the difference between dark, unspoken possibilities and the raw reality of spoken truths. During this phase the context of our family, sometimes covering several generations, is seen and metabolised, understood and given the status of truth according to the client's own sense (ie this is not an idea of reality enforced by the facilitator/therapist, or the representatives in the process of the work, but must only come from the client's own sense of things, which usually takes time).
Our parents were who they are long before we were conceived... we are not the cause of their suffering, but can see that their suffering is theirs, and in a sense nothing to do with us EXCEPT that it had consequences for us.
Seeing this reality does take time, and helps with understanding the why of things: why am I like I am? Why was my mother like she was (and my father)? This context is absolutely crucial and is often what is missing in conventional therapy. Things do not occur out of nothing; there is always a logical context and part of the process of healing is to gain a realistic picture of this context.
Then what?
There comes a phase here, when the person has a more realistic understanding of the context, can discriminate more logically the difference between their own concerns and those of the family, and the question then comes: so now what?
The next logical phase is, with this gained understanding how do I then heal my own trauma? Perhaps I can see more clearly what belongs to my mother and father, and this gives me a better sense of my separateness and individuality, but does this heal my trauma?
The answer is no, it doesn't. Because your trauma is your trauma and understanding the context is only part of the journey. The impact of the context on you, and the way in which you have internalised and been entangled with this context, living it out daily is entirely yours, and in a way this requires a different and more challenging course of action... coming into contact with yourself. Challenging because coming into real contact with yourself means, more than anything, that you will have to experience the split off trauma feelings of terror, despair, desolation, hopelessness and helplessness. In my view it is only then that I can consider my trauma resolved and healed, when I am willing to put myself on the line for myself.
The 'stalled' process
It is often the case that a person may become fixated on the horrors of the context, perhaps keeps interpreting their work in terms of the harm and perpetration done to them by others in the family. This can result in staying a victim, a development of a victim attitude in order to avoid the pain of going further and addressing their own traumatised parts.
There is a moot point in the process of this work where in fact a focus on the context can itself become an easy distraction from this deeper work. A question for the person (and the facilitator) could be: do I really need to keep reliving in this work the perpetration of others to me, or is my continuing concern with these things now an interruption of my healing process?
In the end my trauma is my trauma, and to continue to 'blame' or rage against my mother/father/brother or whoever, avoids the painful experience of connecting with my own traumatised parts. To live on the fact that my mother was a perpetrator is a cop out; to understand that I perpetuate the perpetration against myself, on a daily basis, that I am a continuing perpetrator to myself, is quite another thing.
Bearing in mind that the Trauma of Identity dictates that I must fulfil my mother's wants, not my own, how can I address my own trauma without betraying her? How do I take my eyes off her and her shortcomings and focus on me? How do I dare to put my wants before my identification and compliance with hers? Because, as adult as I am, there is still within me a helpless child, desperately wanting and hoping for the love of my mother, and letting go of this hope is like giving up a life-jacket in the raging ocean: I am sure I will die. To see her really as a perpetrator is desperately painful and like giving up on life itself; for many the unconscious will is 'better some connection with her, to stay in hope, than take the risk that I might die'.
This is not to say however that all that has gone before in the therapy is not absolutely necessary; it is. And along the way, with each insight and shift in perception I am in fact strengthening my healthy 'I', preparing the way for healing. It is also important to know that, in the process, there will be many times when I do come into contact with my traumatised parts, when I do experience some of these feelings and emotions, but the important thing is not to get stuck, to go on, to continue with the started endeavour, not to sidetrack myself but to hold to a growing commitment to myself, to be true to myself, making myself the centre of my world. Because what else is there? What else do I have, really, in my life but myself. I only have others really if I have truly gained myself; I can only really love another if I have felt that real love for myself; I can only really know another, my own children perhaps, if I really am committed to knowing myself.
* I have attempted to vary gender usage, but of course whichever gender terms are used the material also applies to the other.
Write a comment